
قوز قرنیه یا کراتوکونوس (Keratoconus) یکی از شایعترین اختلالات قرنیه است که میتواند بینایی را به طور جدی تحت تاثیر قرار دهد. بسیاری از افراد مبتلا یا کسانی که در خانواده خود سابقه این بیماری را دارند، با این سوال اساسی مواجه هستند که “چه چیزی باعث قوز قرنیه می شود؟” درک علل و عوامل خطر این بیماری، اولین و مهمترین قدم برای مدیریت و پیشگیری از پیشرفت آن است.
پاسخ کوتاه این است که علت دقیق و قطعی قوز قرنیه هنوز به طور کامل شناخته شده نیست. با این حال، تحقیقات گسترده نشان میدهد که این بیماری منشأ چندعاملی دارد؛ یعنی ترکیبی از استعداد ژنتیکی و عوامل محیطی/رفتاری دست به دست هم میدهند تا این اختلال بروز کند. در این مقاله، به طور جامع به تمام عواملی که در ایجاد و تشدید قوز قرنیه نقش دارند، میپردازیم.
قوز قرنیه (کراتوکونوس) به زبان ساده چیست؟
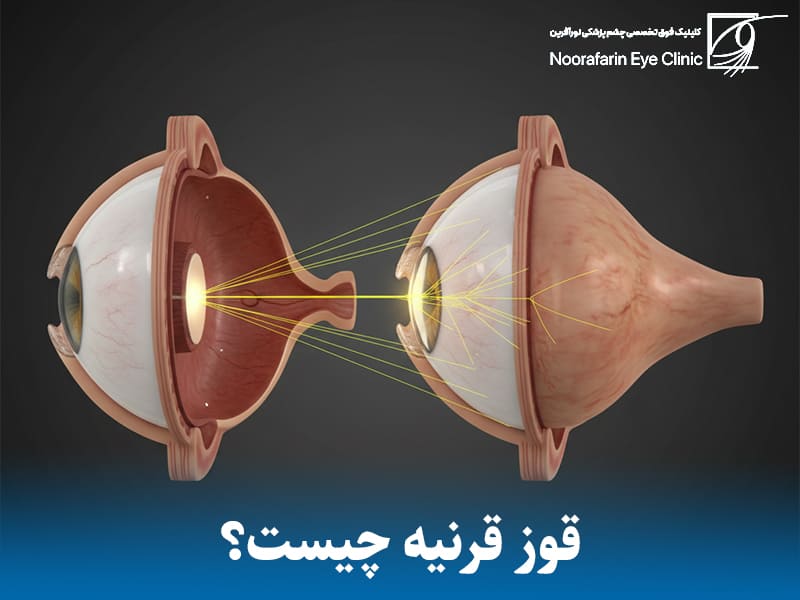
قوز قرنیه یک اختلال چشمی پیشرونده و غیرالتهابی است. در این بیماری، قرنیه (لایه شفاف و گنبدی شکل جلوی چشم) به طور فزایندهای نازک شده و استحکام خود را از دست میدهد. در نتیجه، فشار داخل چشم باعث میشود قرنیه به سمت بیرون برآمده شده و از شکل گرد طبیعی خود به یک شکل مخروطی نامظم (Cone Shape) تغییر حالت دهد.
وظیفه اصلی قرنیه، متمرکز کردن دقیق نور ورودی به چشم بر روی شبکیه است. وقتی شکل قرنیه نامنظم میشود، این تمرکز به هم ریخته و منجر به نزدیکبینی، آستیگماتیسم نامنظم و تاری دید شدید میشود.
- زمان بروز: این بیماری معمولاً در اواخر کودکی یا دوران بلوغ شروع شده و تا اواسط دهه سوم زندگی (۳۰ تا ۴۰ سالگی) به پیشرفت خود ادامه میدهد.
- شیوع: تخمین زده میشود که از هر ۲۰۰۰ نفر، یک نفر به قوز قرنیه مبتلاست، هرچند برخی گزارشها از شیوع بالاتر (تا ۱ در ۴۰۰ نفر) نیز حکایت دارند. متاسفانه، آمار شیوع قوز قرنیه در ایران از میانگین جهانی بالاتر گزارش شده است.
علت قوز قرنیه چیست؟ چه چیزی باعث قوز قرنیه می شود؟
همانطور که اشاره شد، هیچ عامل واحدی به عنوان علت قوز قرنیه شناخته نمیشود. دانشمندان معتقدند این بیماری نتیجه تعامل پیچیده عوامل ژنتیکی و محیطی است.
الف) عوامل ژنتیکی، ارثی و سیستمیک

زمینه ژنتیکی یکی از پایههای اصلی ایجاد بیماری است.
۱. سابقه خانوادگی و وراثت: قوز قرنیه تا حد زیادی یک بیماری ارثی در نظر گرفته میشود. آمارها نشان میدهد که تقریباً از هر ۱۰ بیمار مبتلا، ۱ نفر سابقه خانوادگی مثبت این بیماری را دارد. البته، داشتن ژن بیماری لزوماً به معنای ابتلا نیست؛ اغلب لازم است عوامل محیطی (اپیژنتیک) نیز دخیل باشند تا بیماری بروز کند.
۲. تغییرات بیوشیمیایی در قرنیه: قرنیه از رشتههای پروتئینی به نام کلاژن ساخته شده که استحکام آن را تامین میکنند. در بیماران مبتلا به قوز قرنیه:
- کاهش کلاژن: فرایند از دست رفتن و تخریب کلاژن تسریع میشود.
- کمبود آنتیاکسیدانها: آنتیاکسیدانها وظیفه محافظت از فیبرهای کلاژن را در برابر رادیکالهای آزاد دارند. کمبود آنها باعث ضعیف شدن ساختار کلاژن و برآمدگی قرنیه میشود.
- تغییرات پروتئینی: مطالعات نشان داده که سطح دهها پروتئین مختلف در اشک بیماران مبتلا تغییر میکند که نشاندهنده اختلال در فرآیندهای متابولیکی و سلولی قرنیه است.
۳. بیماریهای همراه (سیستمیک): مشاهده شده است که قوز قرنیه در افراد مبتلا به برخی سندرمها و ناهنجاریهای کروموزومی شایع تر است. این ارتباط قوی، نقش ژنتیک را پررنگتر میکند:
- سندرم داون (Down Syndrome)
- سندرم اهلرز-دانلوس (Ehlers-Danlos Syndrome)
- سندرم مارفان (Marfan Syndrome)
- بیماری رتینیت پیگمانتوزا (Retinitis Pigmentosa)
ب) عوامل محیطی، رفتاری و مکانیکی (عوامل خطر اصلی)

این بخش شاید مهمترین بخش ماجرا باشد، زیرا برخلاف ژنتیک، بسیاری از این عوامل قابل کنترل هستند.
۱. مالش مکرر و مزمن چشم (Eye Rubbing): این مورد به عنوان اصلیترین و قویترین عامل خطر محیطی شناخته میشود. مالیدن محکم و مداوم چشمها، به خصوص با بند انگشت، یک ترومای مکانیکی مزمن به قرنیه ضعیف وارد میکند.
- چرا مالش چشم خطرناک است؟ این کار باعث ضعیف شدن بیشتر پیوندهای کلاژن، کاهش استحکام قرنیه و تسریع روند نازک شدن و برآمدگی آن میشود.
- اهمیت: اگر فردی زمینه ژنتیکی قوز قرنیه را داشته باشد، مالش چشم میتواند مانند یک ماشه عمل کرده و بیماری را آشکار کند یا سرعت پیشرفت آن را به شدت افزایش میدهد.
۲. آلرژیهای چشمی و آتوپی (Atopy): ارتباط بسیار قوی بین قوز قرنیه و سابقه حساسیتهای چشمی، آسم، آلرژی فصلی و اگزما وجود دارد. این ارتباط دوگانه است:
- التهاب: التهاب مزمن ناشی از آلرژی میتواند مستقیماً به بافت قرنیه آسیب بزند.
- خارش: مهمتر از آن، آلرژی باعث خارش شدید چشم میشود و فرد را مجبور به مالش مکرر چشم (عامل شماره ۱) میکند.
۳. آلودگی هوا: تحقیقات جدید نشان میدهد که آلایندههای محیطی مانند ذرات معلق (PM2.5 و PM10) و دیاکسید نیتروژن (NO2) با افزایش شیوع قوز قرنیه همبستگی دارند. این آلایندهها ممکن است با تشدید آلرژی و خشکی چشم، یا به طور مستقیم با آسیب به سلولهای سطح قرنیه (اپیتلیوم)، در بروز بیماری نقش داشته باشند.
۴. کمبود ویتامین D: مطالعات معتبر، ارتباط مستقیمی بین سطح پایین ویتامین D در بدن و افزایش خطر ابتلا یا پیشرفت سریعتر قوز قرنیه پیدا کردهاند.
۵. خشکی چشم: خشکی شدید سطح چشم، به دلیل ایجاد التهاب و همچنین افزایش تمایل فرد به مالش چشم، به عنوان یک ریسک فاکتور مطرح شده است.
۶. سایر عوامل:
- نحوه خوابیدن: خوابیدن به صورت دمر (رو به شکم) که باعث ایجاد فشار مکانیکی طولانیمدت روی قرنیه میشود.
- تابش UV: قرار گرفتن طولانیمدت در معرض اشعه فرابنفش خورشید بدون محافظت (عینک آفتابی).
عوامل خطر و عوامل محافظتی قوز قرنیه
برای درک بهتر، عوامل موثر بر قوز قرنیه را میتوان در جدول زیر خلاصه کرد:
| دستهبندی | عوامل خطر (افزایشدهنده ریسک) | عوامل محافظتی (کاهشدهنده ریسک) |
|---|---|---|
| ژنتیکی | سابقه خانوادگی مثبت (۱ در ۱۰ مورد) | – |
| سیستمیک | سندرم داون، مارفان، اهلرز-دانلوس | بیماری دیابت (به طور جالب توجهی) |
| رفتاری | مالش مکرر و مزمن چشم (عامل اصلی) | ترک کامل عادت مالش چشم |
| محیطی | آلرژیهای چشمی، آسم، اگزما | درمان آلرژی و خشکی چشم |
| محیطی | آلودگی هوا (PM2.5, NO2) | استفاده از عینک آفتابی (محافظت از UV) |
| رفتاری | خوابیدن به صورت دمر (رو به شکم) | خوابیدن به پشت یا پهلو |
| تغذیهای | کمبود ویتامین D | حفظ سطح نرمال ویتامین D |
علائم و نشانههای قوز قرنیه چیست؟
با پیشرفت بیماری و تغییر شکل قرنیه، علائم زیر به تدریج ظاهر میشوند:
- تاری دید و اعوجاج (کج و معوج دیدن خطوط صاف)
- نزدیکبینی و آستیگماتیسم نامنظم که به سرعت پیشرفت میکند
- نیاز مداوم به تعویض نمره عینک
- افزایش حساسیت شدید به نور (فتوفوبیا)
- مشاهده هاله (Halo) در اطراف منابع نوری (مانند چراغها در شب)
- دوبینی (حتی با یک چشم)
- خستگی چشم و سردردهای مرتبط
در موارد بسیار پیشرفته، ممکن است پارگی ناگهانی در لایههای داخلی قرنیه رخ دهد (هیدروپس قرنیه) که باعث درد، تورم و کاهش دید ناگهانی و شدید میشود.
روش های درمان قوز قرنیه (بر اساس شدت بیماری)
درمان قوز قرنیه به شدت بیماری، سرعت پیشرفت آن و نیازهای بینایی بیمار بستگی دارد. اهداف اصلی درمان دو مورد هستند: ۱) متوقف کردن پیشرفت بیماری و ۲) بهبود کیفیت بینایی.
مرحله اول: اصلاح دید در مراحل اولیه
در مراحل خفیف بیماری، تمرکز بر اصلاح آستیگماتیسم نامنظم است.
- عینک (Eyeglasses): در ابتداییترین مراحل، عینک میتواند تاری دید و نزدیکبینی را اصلاح کند. با این حال، با پیشرفت بیماری، نمره عینک به سرعت تغییر کرده و دیگر قادر به ایجاد دید واضح نخواهد بود.
- لنزهای تماسی نرم (Soft Contact Lenses): لنزهای نرم توریک (Toric) مخصوص آستیگماتیسم نیز میتوانند در موارد خفیف موثر باشند.
مرحله دوم: لنزهای تخصصی برای مراحل متوسط
زمانی که عینک دیگر دید کافی را فراهم نمیکند، لنزهای تخصصی بهترین گزینه هستند.
- لنزهای سخت نفوذپذیر به گاز (RGP – Rigid Gas Permeable): این لنزها اولین خط درمان برای اکثر بیماران هستند. لنزهای RGP سطح سفتی دارند و شکل نامنظم قرنیه را نمیپوشانند، بلکه یک سطح انکساری صاف و جدید در جلوی قرنیه ایجاد میکنند. فضای بین لنز و قرنیه با اشک پر میشود که آستیگماتیسم نامنظم را خنثی کرده و دید بسیار شفافی ایجاد میکند. تحمل این لنزها در ابتدا ممکن است کمی دشوار باشد.
- لنزهای اسکلرال (Scleral Lenses): این لنزها انقلابی در درمان قوز قرنیه ایجاد کردهاند. لنزهای اسکلرال قطور و بزرگ هستند و به جای قرار گرفتن روی قرنیه حساس، به طور کامل روی سفیدی چشم (صلبیه) قرار میگیرند و مانند یک پل از روی قرنیه عبور میکنند. فضای زیر لنز با اشک مصنوعی پر شده و تمام نامنظمیهای قرنیه را میپوشاند. این لنزها دیدی عالی همراه با راحتی فوقالعاده (حتی راحتتر از لنزهای نرم) فراهم میکنند و برای موارد متوسط تا شدید ایدهآل هستند.
- لنزهای هیبریدی (Hybrid Lenses): این لنزها دارای یک مرکز سخت (مانند RGP) برای ایجاد دید شفاف و یک حاشیه نرم (Skirt) برای راحتی بیشتر هستند.
مرحله سوم: توقف پیشرفت بیماری (کراس لینکینگ)
این روش، حیاتیترین اقدام برای بیماران در حال پیشرفت است.
- پیوند متقابل کلاژن قرنیه (Corneal Cross-Linking – CXL): این یک روش درمانی (و نه زیبایی) است که هدف آن متوقف کردن یا کند کردن روند پیشرفت قوز قرنیه است. CXL دید را به طور قابل توجهی بهبود نمیدهد، بلکه قرنیه را مستحکم میکند تا از بدتر شدن بیماری و نیاز به پیوند قرنیه در آینده جلوگیری کند.
- روش کار: در این عمل سرپایی، ویتامین B2 (ریبوفلاوین) به صورت قطره روی قرنیه ریخته شده و سپس نور ماوراء بنفش (UV) کنترل شده به آن تابانده میشود. این فرایند باعث ایجاد پیوندهای متقاطع جدید و قوی بین رشتههای کلاژن قرنیه شده و ساختار آن را تقویت میکند.
مرحله چهارم: جراحیهای اصلاحی و نهایی (مراحل پیشرفته)
زمانی که بیماری شدید است یا بیمار قادر به تحمل لنز نیست، گزینههای جراحی مطرح میشوند.
- کاشت رینگهای داخل قرنیه (Intacs / Keraring): در این روش، یک یا دو حلقه پلاستیکی نازک (C-shaped) در لایههای میانی قرنیه (استروما) کاشته میشوند. این رینگها با فشار آوردن به محیط قرنیه، مرکز آن را صافتر کرده و شکل مخروطی را کاهش میدهند. این کار به بهبود آستیگماتیسم، بهبود بینایی و گاهی تحمل بهتر لنز کمک میکند. این روش معمولاً با CXL ترکیب میشود.
- پیوند قرنیه (Corneal Transplant / Keratoplasty): این روش آخرین راهحل برای درمان قوز قرنیه است و زمانی انجام میشود که قرنیه دچار کدورت شدید (اسکار)، نازکی بیش از حد شده باشد و یا هیچ لنزی نتواند دید مفیدی را فراهم کند.
- پیوند لایهای عمیق قدامی (DALK): در این روش ترجیحی، تنها لایههای سطحی و میانی قرنیه بیمار برداشته شده و با بافت اهدایی جایگزین میشود، اما داخلیترین لایه (اندوتلیوم) خود بیمار حفظ میشود. این کار خطر رد پیوند را به شدت کاهش میدهد.
- پیوند تمام ضخامت (PKP): در این روش، کل ضخامت قرنیه بیمار با قرنیه اهدایی تعویض میشود. نکته مهم: حتی پس از پیوند قرنیه موفق، اکثر بیماران برای دستیابی به دید کامل، همچنان به عینک یا لنزهای تماسی (اغلب اسکلرال) نیاز خواهند داشت.
قوز قرنیه و جراحیهای لیزری (لیزیک، لازک)
یک نکته حیاتی که تمام افراد باید بدانند: انجام عملهای جراحی لیزری عیوب انکساری (مانند لیزیک، لازک، و PRK)، که اغلب با عناوینی چون عمل حذف عینک مشهد جستجو میشوند، برای افراد مبتلا به قوز قرنیه یا حتی مشکوک به آن، مطلقاً ممنوع است.
این جراحیها با نازک کردن قرنیه، بیماری را به شدت تشدید کرده و میتوانند منجر به عارضه خطرناکی به نام “اکتازی پس از عمل” شوند که درمان آن بسیار دشوار است.
تشخیص دقیق قوز قرنیه پنهان (Forme Fruste) قبل از هرگونه عمل لیزری، توسط توپوگرافی قرنیه، الزامی است. این ارزیابی تخصصی باید در مراکزی انجام شود که تجهیزات کامل تشخیصی قرنیه را دارند، مانند مواردی که در جستجوی بهترین کلینیک چشم پزشکی در مشهد یا سایر شهرهای بزرگ یافت میشوند.
علت و علائم قوز قرنیه چیست و چگونه درمان می شود؟
قوز قرنیه یک بیماری چندعاملی است که در آن ژنتیک زمینه را فراهم کرده و عوامل محیطی (به ویژه مالش چشم و آلرژی) آن را شعلهور میسازند. اگرچه نمیتوانیم ژنتیک خود را تغییر دهیم، اما میتوانیم عوامل خطر محیطی را به طور کامل کنترل کنیم.
مهمترین توصیه: ۱. هرگز چشمان خود را نمالید. ۲. آلرژی و خشکی چشم خود را به طور جدی درمان کنید. ۳. در صورت داشتن سابقه خانوادگی یا علائمی مانند تاری دید و تغییر سریع نمره عینک، فوراً برای ارزیابی دقیق (به خصوص توپوگرافی قرنیه) به چشم پزشک یا اپتومتریست مراجعه کنید. تشخیص زودهنگام، چه در پایتخت و چه در جستجوی بهترین دکتر فوق تخصص چشم در مشهد، کلید مدیریت موفقیت آمیز این بیماری است.







8 پاسخ
سلام آقای دکتر، خسته نباشید. مقاله رو خوندم خیلی کامل بود. من خودم قوز قرنیه دارم و ۳۵ سالمه. خیلی نگران دختر ۵ سالهم هستم. آیا الان لازمه بیارمش برای معاینه؟ یا صبر کنم بزرگتر بشه؟ خیلی میترسم اونم مثل من بشه.
سلام مریم عزیز. نگرانی شما کاملاً طبیعی است، اما استرس نداشته باشید. همانطور که در مقاله اشاره کردیم، وراثت نقش دارد اما قطعی نیست. برای کودکان با سابقه خانوادگی، پیشنهاد میکنیم از سنین مدرسه (۶-۷ سالگی) معاینات سالانه انجام شود. مهمترین نکته برای دختر گلتان این است که نگذارید چشمانش را بمالد (مخصوصاً اگر آلرژی دارد). مالش چشم ماشه اصلی این بیماری است. در پناه خدا باشید.
وقت بخیر. ممنون بابت توضیحات. من چشم چپم نیاز به عمل رینگ داره طبق نظر پزشکم. خواستم بدونم هزینه عمل رینگ داخل قرنیه تو کلینیک نورآفرین چقدره و آیا بیمه تکمیلی قبول میکنید؟
سلام آقا محسن عزیز. خوشحالیم که همراه ما هستید. هزینه عمل بسته به نوع رینگ مصرفی و شرایط چشم شما متغیر است. بله، کلینیک نورآفرین با اکثر بیمههای تکمیلی قرارداد دارد. برای اطلاع دقیق از تعرفههای سال ۱۴۰۴ و مشاوره بیمه، لطفاً با شمارههای موجود در سایت (۳۱۷۱۶-۰۵۱) تماس بگیرید یا در واتساپ پیام دهید تا همکارانم راهنماییتان کنند.
دکتر جان من هفته دیگه نوبت عمل کراس لینکینگ دارم ولی وحشتناک از دردش میترسم. شنیدم بعد عمل خیلی درد داره. حقیقت داره؟ میشه کاری کرد دردش کمتر بشه؟
سلام سارای عزیز. اصلا نگران نباشید. عمل کراس لینکینگ (CXL) یکی از کمخطرترین عملهاست. حین عمل که با قطره بیحسی هیچ دردی حس نمیکنید. بعد از عمل ممکن است ۱ تا ۲ روز سوزش و اشکریزش داشته باشید که کاملاً طبیعی است و با لنز پانسمان و مسکنهایی که تجویز میکنیم، کاملاً قابل کنترل است. استرس خودش درد را بیشتر میکند، پس با آرامش کامل تشریف بیاورید.
سلام. ببخشید یه سوال داشتم که شاید سوال خیلیها باشه. من نمره چشمم بالاست و قوز قرنیه دارم. آیا با قوز قرنیه میتونم معافیت سربازی بگیرم؟ شدت بیماریم متوسطه.
سلام امیرعلی جان. بله، قوز قرنیه یکی از موارد شامل معافیت پزشکی است، اما بستگی مستقیم به شدت بیماری و نتایج توپوگرافی قرنیه دارد. معمولاً اگر بیماری پیشرفته باشد و دید را به شدت مختل کرده باشد، شامل معافیت دائم میشود. پیشنهاد میکنم یک نوبت معاینه رزرو کنید تا با بررسی دقیق عکس قرنیه، وضعیت شما را برای کمیسیون پزشکی ارزیابی کنیم.